VHL is by in large an inherited rare disorder. It is an autosomal dominant disease and about 20% of people with VHL have a de novo mutation [first in family]. It is estimated that 1 in 36,000 people have VHL, with approximately 10,000 individuals living with VHL disease in the United States [and about 900 in Canada].
The VHL gene mutation and the resulting over expression of the HIF protein produce both nonmalignant and malignant tumors. Tumors can develop in up to ten different parts of the body, at any time throughout a patient’s lifetime. This process can start as early as 1 years of age. Patients often describe VHL as having cancer again, and again, and again.
VHL-related tumors can [re] occur in the brain, spine, kidney, pancreas, adrenals, retina, endolymphatic sac, broad ligament, epididymis, liver and lung. Multiple lesions in any given organ are common...
Treatment and monitoring involves specialist appointments, multi-care clinics, tests (e.g. MRI), surgeries, dialysis, medication, rehabilitation and other procedures for reoccurring tumours in common areas such as the brain, spine, eyes, kidneys, and pancreas...
The VHL gene mutation and the resulting over expression of the HIF protein produce both nonmalignant and malignant tumors. Tumors can develop in up to ten different parts of the body, at any time throughout a patient’s lifetime. This process can start as early as 1 years of age. Patients often describe VHL as having cancer again, and again, and again.
VHL-related tumors can [re] occur in the brain, spine, kidney, pancreas, adrenals, retina, endolymphatic sac, broad ligament, epididymis, liver and lung. Multiple lesions in any given organ are common...
Treatment and monitoring involves specialist appointments, multi-care clinics, tests (e.g. MRI), surgeries, dialysis, medication, rehabilitation and other procedures for reoccurring tumours in common areas such as the brain, spine, eyes, kidneys, and pancreas...
BRAIN AND SPINAL CORD
Lesions or hemangioblastomas in the CNS are benign. However, the pressure on the brain and/or spinal cord by growing tumors and cysts can result in various symptoms including severe back pain, headaches, numbness, dizziness, bowel/bladder incontinence, increased reflexes, incoordination and/or weakness or pain in the arms and legs. Depending on location, excision can be challenging, particularly if the tumor is located in the brain stem or is intertwined with the spinal cord. Of note, excisions of CNS hemangioblastomas are the leading cause of VHL morbidity and mortality.
KIDNEY
VHL kidney tumors are clear cell renal carcinomas (ccRCC), which, if allowed to grow greater than approximately 3 cm, will become metastatic. An organ sparing approach to excision is the preferred strategy for ensuring that a patient will have sufficient kidney function throughout their lifetime. Diminished kidney function is accompanied with each surgical intervention, which can lead to the need for dialysis or transplantation.
PANCREAS
There are three types of VHL lesions that can be occur in the pancreas: cysts, serous microcystic adenomas or “cystadenomas,” and pancreatic neuroendocrine tumors (pNETs). All can cause functional problems as well as structural problems. Unless the cysts or cystadenomas are positioned such that there is loss of pancreatic function, they generally do not require surgical intervention. On the other hand, pNETs can become metastatic if the patient’s VHL mutation is on exon 3. Like for the kidney, multiple surgical interventions can lead to a loss of pancreatic function resulting in hormonal insufficiency, including decreased insulin production. It is also not uncommon for a Whipple procedure to be required to remove pNETs in VHL patients.
ADRENAL GLANDS
Pheochromocytomas (“pheos”), which are tumors of the adrenal glands, are rarely malignant. It is the resulting elevated levels of normetanephrine that can be dangerous and life-threatening for VHL patients. The excessive amounts of adrenaline cause spiking blood pressure putting strain on the heart and vascular system. Symptoms can also include headaches, irregular or rapid heartbeat, or what feels like a panic attack, fear, anxiety, or, even, rage. In order to eliminate the risk created by elevated normetanephrines excision of active pheos is imperative. While partial adrenalectomies are the preferred approach, they are not always possible and therefore radical adrenalectomies are performed. multiple partial adrenalectomies and radical adrenalectomies result in the need for a life of adrenal hormone supplementation. Monitoring the fine balance of hormones is essential to avoid adrenal crisises.
EYE - RETINA
Hemangioblastomas of the retina can often be treated with minimal vision loss and risk. Small lesions are treated with laser surgery while larger lesions are treated with cryotherapy. If not addressed immediately or properly, retinal hemangioblastomas can lead to a detached retina, or vitreous hemorrhage. In this situation, vitrectomy or scleral buckling are the most appropriate treatment options. Unfortunately, there are few treatments available for lesions on the optic disc. It is not uncommon for patients to experience so many retinal hemangioblastomas that they become blind.
INNER EAR
Endolymphatic sac tumors (ELSTs) can form behind the inner ear. Symptoms include tinnitus, dizziness, balance issues, fullness in an ear, or facial weakness, subtle changes in the “texture” of the hearing to profound hearing loss. Hearing loss may occur suddenly or gradually over a period of 6 months. Once hearing is lost, it is very difficult, if not impossible, to regain. Tumors as small as 2 mm found during surgery have been found to affect hearing. Excision is required to remove the tumor in order to prevent further hearing loss.
REPRODUCTIVE
Epididymal and broad ligament cystadenomas are additional manifestations for male and female VHL patients, respectively. While infertility can ensue, these benign tumors generally do not require surgical intervention.
OTHER
VHL has been associated with benign asymptomatic cysts in the lungs and liver. There is no reason to believe that these lesions are of concern. However, there presence cause additional anxiety on the patient.
VHL Alliance - FDA Listening Session - June 11, 2020
Overview of VHL: Eric Jonasch, MD, Professor, Department of Genitourinary Medical Oncology, Division of Cancer Medicine, The University of Texas MD Anderson Cancer Center
Lesions or hemangioblastomas in the CNS are benign. However, the pressure on the brain and/or spinal cord by growing tumors and cysts can result in various symptoms including severe back pain, headaches, numbness, dizziness, bowel/bladder incontinence, increased reflexes, incoordination and/or weakness or pain in the arms and legs. Depending on location, excision can be challenging, particularly if the tumor is located in the brain stem or is intertwined with the spinal cord. Of note, excisions of CNS hemangioblastomas are the leading cause of VHL morbidity and mortality.
KIDNEY
VHL kidney tumors are clear cell renal carcinomas (ccRCC), which, if allowed to grow greater than approximately 3 cm, will become metastatic. An organ sparing approach to excision is the preferred strategy for ensuring that a patient will have sufficient kidney function throughout their lifetime. Diminished kidney function is accompanied with each surgical intervention, which can lead to the need for dialysis or transplantation.
PANCREAS
There are three types of VHL lesions that can be occur in the pancreas: cysts, serous microcystic adenomas or “cystadenomas,” and pancreatic neuroendocrine tumors (pNETs). All can cause functional problems as well as structural problems. Unless the cysts or cystadenomas are positioned such that there is loss of pancreatic function, they generally do not require surgical intervention. On the other hand, pNETs can become metastatic if the patient’s VHL mutation is on exon 3. Like for the kidney, multiple surgical interventions can lead to a loss of pancreatic function resulting in hormonal insufficiency, including decreased insulin production. It is also not uncommon for a Whipple procedure to be required to remove pNETs in VHL patients.
ADRENAL GLANDS
Pheochromocytomas (“pheos”), which are tumors of the adrenal glands, are rarely malignant. It is the resulting elevated levels of normetanephrine that can be dangerous and life-threatening for VHL patients. The excessive amounts of adrenaline cause spiking blood pressure putting strain on the heart and vascular system. Symptoms can also include headaches, irregular or rapid heartbeat, or what feels like a panic attack, fear, anxiety, or, even, rage. In order to eliminate the risk created by elevated normetanephrines excision of active pheos is imperative. While partial adrenalectomies are the preferred approach, they are not always possible and therefore radical adrenalectomies are performed. multiple partial adrenalectomies and radical adrenalectomies result in the need for a life of adrenal hormone supplementation. Monitoring the fine balance of hormones is essential to avoid adrenal crisises.
EYE - RETINA
Hemangioblastomas of the retina can often be treated with minimal vision loss and risk. Small lesions are treated with laser surgery while larger lesions are treated with cryotherapy. If not addressed immediately or properly, retinal hemangioblastomas can lead to a detached retina, or vitreous hemorrhage. In this situation, vitrectomy or scleral buckling are the most appropriate treatment options. Unfortunately, there are few treatments available for lesions on the optic disc. It is not uncommon for patients to experience so many retinal hemangioblastomas that they become blind.
INNER EAR
Endolymphatic sac tumors (ELSTs) can form behind the inner ear. Symptoms include tinnitus, dizziness, balance issues, fullness in an ear, or facial weakness, subtle changes in the “texture” of the hearing to profound hearing loss. Hearing loss may occur suddenly or gradually over a period of 6 months. Once hearing is lost, it is very difficult, if not impossible, to regain. Tumors as small as 2 mm found during surgery have been found to affect hearing. Excision is required to remove the tumor in order to prevent further hearing loss.
REPRODUCTIVE
Epididymal and broad ligament cystadenomas are additional manifestations for male and female VHL patients, respectively. While infertility can ensue, these benign tumors generally do not require surgical intervention.
OTHER
VHL has been associated with benign asymptomatic cysts in the lungs and liver. There is no reason to believe that these lesions are of concern. However, there presence cause additional anxiety on the patient.
VHL Alliance - FDA Listening Session - June 11, 2020
Overview of VHL: Eric Jonasch, MD, Professor, Department of Genitourinary Medical Oncology, Division of Cancer Medicine, The University of Texas MD Anderson Cancer Center
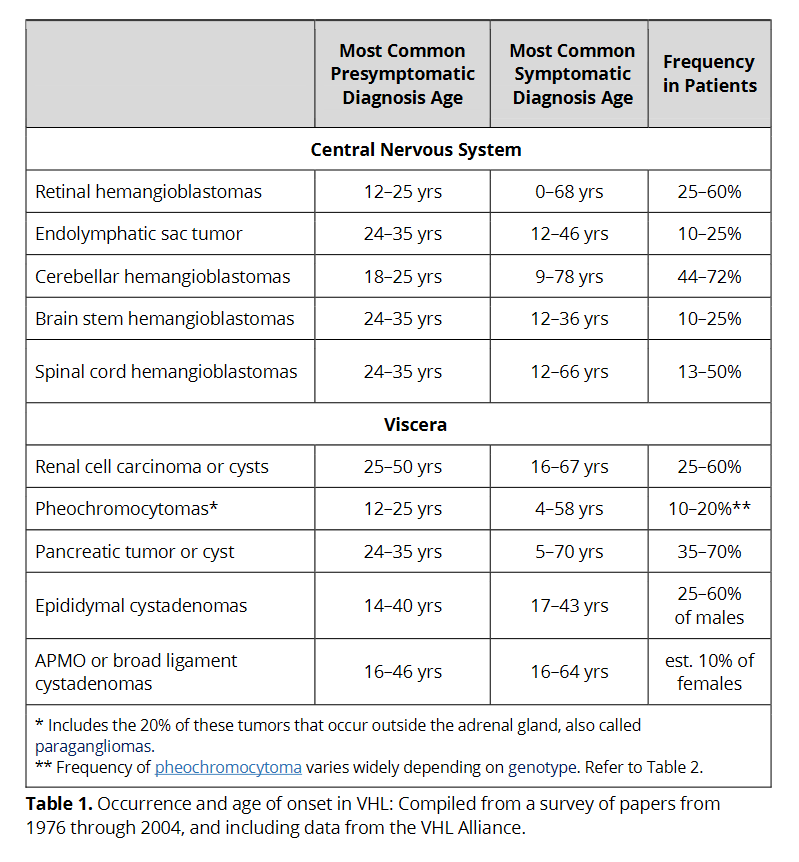
"Occurrance and onset of VHL" from VHL Alliance Patient Handbook (2020):